
Abstract
Background
Falls are a serious problem in the elderly, and have recently been described as cardiovascular-mediated side effects of beta-blocker eye drops. Therefore, we investigated the possible association between the long-term use of beta-blockers, prostaglandins and their combinations in eye drops, and falls, dizziness and orthostatic hypotension in older patients.
Methods
All participants were long-term users of eye drops containing beta-blockers, prostaglandins or their combinations. They underwent a structured falls interview and blood pressure measurement for testing of orthostatic hypotension. The odds ratio for presence of orthostatic hypotension or a positive falls history according to use of beta-blocker eye drops was calculated with a binary logistic regression analysis. The main outcome measures were a positive falls history and the presence of orthostatic hypotension.
Results
In total, 148 of 286 subjects participated. After adjustment for age, gender, and use of fall-risk-increasing drugs other than beta-blocker eye drops, we found no significant difference in fall risk [odds ratio (OR): 0.60; 95% confidence interval (CI): 0.268–1.327] between patients using ophthalmic beta-blockers or a combination of ophthalmic beta-blockers and prostaglandins, and patients using ophthalmic prostaglandins only. Although prevalence of orthostatic hypotension was higher in the beta-blocker group (OR: 1.67; 95% CI: 0.731–3.793) compared to the prostaglandin group, this was a non-significant difference.
Conclusions
In our study, we did not find a significant association between long-term use of beta-blockers eye drops and falls, dizziness or orthostatic hypotension in older ophthalmic outpatients, compared to long-term use of prostaglandin eye drops.
Similar content being viewed by others


Introduction
Many ophthalmic diseases are more common in the ageing eye. One of them is glaucoma, for which current treatment is based on lowering intraocular pressure (IOP) [1, 2]. Nowadays there is a wide range of topical medication available. One of the older, but still frequently prescribed topical drugs is timolol, which is a non-selective beta-adrenoceptor antagonist without intrinsic sympathicomimetic activity. Blockading of beta-receptors leads to a decrease of aqueous formation and lowering of the IOP [3].
With respect to cardiovascular and pulmonary systemic side-effects, many reports have been published in the literature. In a study in which the dose and effect of oral and topical beta-blockers were compared, the systemic (side-)effects of topical timolol were the same as those associated with oral timolol [4].
For newer drugs, such as the prostaglandin analogs, and for carbonic anhydrase inhibitors, no cardiovascular side-effects are known [5–7]. Therefore, nowadays many ophthalmologists are considering exclusion of the (cheap and effective) beta-blocker as a first-line drug in the treatment of glaucoma, in favor of the new (and more expensive) prostaglandin analogs.
Recently, falls induced by beta-blocker eye drops have been described as cardiovascular-mediated adverse drug reactions [8]. Falls are a serious problem in the elderly, and are associated with increased morbidity and mortality. They can lead to reduced functioning and early admissions to nursing homes and long-term care facilities, but also to a reduced quality of life [9]. Polypharmacy and the use of certain (groups of) drugs have been found to be associated with an increased risk of falling [10–12]. Withdrawal of these drugs can result in a reduction of fall risk [13, 14].
Several case reports have described patients in whom (recurrent) syncope was probably caused by beta-blocker eye drops such as timolol, supporting an advice for re-consideration of the usefulness and safety of topical beta-blockers [8, 15, 16]. However, before we stop prescribing beta-blocker eye drops, more research is needed to determine whether these glaucoma medications indeed constitute a higher risk of falling compared to the newer prostaglandins [17]. Many clinical trials suggest a better IOP-lowering effect of prostaglandins compared to beta-blockers; however, some recent (meta-analysis) studies found a similar effect of the mentioned eye drops [18, 19]. Exclusion of timolol would thus mean the loss of a very potent and cheap IOP-lowering drug, and an increase in costs of glaucoma treatment. Therefore we set out to analyze the possible association between the long-term use of beta-blocker eye drops, and falls and orthostatic hypotension in older outpatients of the ophthalmology outpatient clinic of the Erasmus University Medical Center.
Methods
This cross-sectional study was performed at the outpatient clinic of the Department of Ophthalmology of the Erasmus University Medical Center, Rotterdam, the Netherlands. The Medical Ethics Committee of the Erasmus University Medical Center approved the study.
Study participants and methods
The inclusion criteria were: age 60 years or older, diagnosis of ocular hypertension or open-angle glaucoma, use of topical treatment to lower intraocular pressure for at least 1 year, and most recent visit within the past year. Eligible topical medication was defined as beta-blockers, prostaglandin analogs or combination products with at least one of the two aforementioned components. Single use of all other topical medication for lowering intraocular pressure was excluded, because of the very low numbers of patients and possible systemic side-effects like dizziness and systemic hypotension [5, 6].
Subjects fulfilling the inclusion criteria were sent an information letter by post. One week later, we contacted them by phone to give further information. If the patient so wished, an appointment was made for a regular visit to our outpatient clinic, for an assessment. The assessment consisted of a structured interview, including questions regarding frequency and probable causes of falling in the last 12 months, and an inventory of all current medication.
Physical examination consisted of blood pressure and pulse rate measurements after 10 minutes in a supine position. Next, the patient was asked to stand up so we could measure the blood pressure and pulse rate in an upright position after 1, 2, 3 and 5 minutes.
Outcome definition
Two separate outcomes were defined, a positive history of falling, and the presence of orthostatic hypotension respectively. Fall incidents were defined as coming to rest unintentionally on the ground or a lower level with or without losing consciousness [20]. A positive falls history was defined as occurrence of a fall incident within the past 12 months.
Orthostatic hypotension was defined as a decrease of 20 mmHg in systolic and/or 10 mmHg in diastolic blood pressure on standing [21]. Blood pressure and pulse rate were measured with a Datascope Accutorr Plus NIBP with Trend Screen (Datascope Corp., USA). This device has demonstrated acceptable accuracy and precision for measuring blood pressure [22, 23].
Statistical analysis
We created three groups of patients: a group on eye drops with beta-blocker (without prostaglandin), a group on combination therapy (with prostaglandin) and, as the reference group, the group on prostaglandins. In the analyses, we combined the beta-blocker and the combination group as one group of beta-blocker users. Baseline differences between the subgroups were tested using an independent t-test and a chi-square test.
We analyzed the association of falling and the use of beta-blocker eye drops using a binary logistic regression model, and calculated odds ratios with corresponding 95% confidence intervals, which can be interpreted as estimators of relative risks. The results were adjusted for age, gender and number of fall-risk-increasing drugs (FRID). FRID included psychotropic drugs (sedatives, antidepressants, neuroleptics), cardiovascular drugs [antihypertensives (including oral beta-blockers), nitrates, anti-arrhytmics] and analgesics, hypoglycemics and urinary antispasmodics [14].
For differences in blood pressure and pulse rate between the mentioned groups we used the Student’s t-test. Analyses were performed using SPSS (Statistical Package for the Social Sciences) 15.0.0 (SPSS Inc., Chicago, IL, USA; 2006).
Results
Of the 286 eligible subjects, 148 agreed and were able to participate in the time-frame of our study (mean age 73.7 years, range 61–91 years). The other 138 patients could either not be contacted (N = 56), or were unable to participate for several reasons: too difficult to get to the clinic (N = 27), illness (N = 17), poor command of the Dutch language (N = 5), unknown (N = 13), other reasons (N = 20). The non-responders were on average 3 years older (p = 0.002 adjusted for gender).
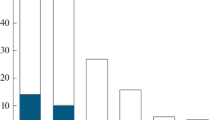
The patients’ general characteristics are shown in Table 1. The mean duration of usage of topical ophthalmic medication without changes in prescription was 2.87 years (range 1–13 years). Figure 1 shows the type and percentages of topical medications in our study.

Eye drops used, and their groups, with total frequencies of population. (Types of eye drop for lowering intraocular pressure)
Of the 148 subjects, 41 (27.7%) reported at least one fall in the past year. Of those, 19 (12.8%) were multiple fallers, of whom nine used beta-blocker eye drops. Prevalence of falling was not significantly different between men and women [odds ratio (OR) for females 1.39; 95% confidence interval (CI): 0.664–2.909 compared to males; adjusted for age and number of FRID].
Mean number of prescribed drugs used by subjects, including injections (insulin, vitamin B-12) and eye drops, was 5.09 (range 1–16). The risk of a positive falls history did not increase with the number of different medications used. Mean number of FRID use was 2.02 (range 0–12). We found a significant higher risk of falling for the number of FRIDs (OR 1.20; 95% CI: 1.017–1.407 adjusted for age and gender), but not specifically for the ophthalmic medication under study.
The results on risk of falling and complaints of dizziness on beta-blocker eye drops are displayed in Table 2. There were no statistically significant differences between the groups for falls or dizziness, suggesting that there is no higher risk of falling or dizziness with long-term use of topical beta-blockers. As falling seems related to visual field status, we added visual field data (mean deviation) to the model, but that did not statistically significantly change the risk estimate (OR 0.63; 95% CI 0.244–1.605). The risk of falling increased slightly (OR 0.76; 95% CI 0.329–1.740) if we combined the oral beta-blockers and eye drops versus the group without any beta-blocker use (‘clean’ group). This was not the case for the other two outcomes.
Mean blood pressures were similar in the defined subgroups. The mean systolic and diastolic blood pressure increased significantly (p < 0.001) between 1 and 2 minutes in upright position. Orthostatic hypotension occurred in 39 subjects (26.4%), of whom 15 cases (23.8%) were in the prostaglandin group and 24 cases (28.2%) in the beta-blocker group. We found no significant difference in risk of orthostatic hypotension for beta-blocker use (OR 1.67; 95% CI 0.731–3.793). If we subdivided the beta-blocker group into a beta-blocker [N (%) = 12 (33.3%)] and a combination group [N (%) = 12(24.5%)], we found an OR of 2.32 (95% CI 0.845–6.345) and of 1.34 (95% CI 0.532–3.382) respectively, compared to the prostaglandin group (both adjusted for age, gender and number of FRID).
Figure 2 shows that the mean pulse rate in the group on beta-blocker eye drops was lower than for the combination group, and both are lower than mean pulse rate for the subjects using only prostaglandin eye drops. The pulse rate increased significantly (p < 0.001) in all subgroups in the period after 10 minutes in supine position to 1 minute in upright position. The increase in the pulse rate at 1 minute of standing was significantly lower (p < 0.05) in the beta-blocker group than in the prostaglandin group. However, we found no significant difference for the other measured time points, neither for the beta-blocker group nor for the group using combination drugs compared to the prostaglandin group. There were eight patients (5.4%) with an irregular pulse rate. Of those, five (7.9%) used a prostaglandin, one (2.8%) a beta-blocker and two (4.1%) combination therapy.

Mean pulse rates. (u.p. = upright position)
Discussion
The results of our study suggest that stable long-term use of beta-blocker eye drops is not associated with an increased risk in falling or dizziness in comparison to the use of prostaglandin eye drops in older patients with ocular hypertension or glaucoma. This is in contrast with other studies, possibly because we studied the long-term users of topical beta-blockers. Furthermore, there may be an increased risk of orthostatic hypotension, although in our study this did not reach statistical significance. However, we did find a significantly lower increase in pulse rate after 1 minute of standing in topical beta-blocker users, which, in daily life, may contribute to fall risk on standing up.
As mentioned earlier, treatment of glaucoma is based on lowering IOP with topical medication. Timolol was one of the first topical drugs available for the treatment of elevated IOP, with only a few ocular side-effects. It revolutionized the medical therapy of glaucoma at the end of the 1970s. Now, almost 30 years later, it still remains a frequently prescribed IOP-lowering drug, even though by now many systemic (side-)effects have been identified; in the worst case, an adverse event can lead to death [7, 24]. There are four types of side-effects of beta-blockers: cardiovascular (heart failure, arrhythmia, altering serum lipids, decrease in blood pressure), pulmonary [exacerbation of reactive airways disease (asthma, COPD)], central nervous system (headaches, weakness, depression) and endocrine (hypoglycemia in diabetes) [3, 7, 24–28]. Several studies suggest that the prevalence of these side-effects is less common in selective topical beta-blocker (betaxolol) [7, 17, 25, 29], but the contrary has also been shown [30, 31].
At least 80% of the administered eye drop can be absorbed into conjunctival, nasal (through the nasolacrimal duct), oropharyngeal and gastrointestinal mucosa and cause systemic side-effects [7, 8]. There is no hepatic first-pass effect, therefore topical administration “mimics” intravenous rather than oral administration. Two drops of a 0.5% standard dose of timolol in one eye each can approximate to a 10 mg oral dose to treat systemic hypertension [3, 24, 29].
There is a considerable variation in the degree of systemic absorption between individuals. Older individuals have also a slower metabolism of pharmaceuticals and can thus reach higher plasma levels. However, cardiovascular side-effects of timolol eye drops have been reported at low plasma levels (<2.8 ng/ml) [32] and even at undetectable plasma levels (<1.0 ng/ml) [32, 33]. This is probably due to the long-lasting occupancy of the beta-receptors by their antagonists in elderly patients [34].
Pharmacokinetic studies have shown that only 1–7% of the administered eye drop penetrates the cornea and that the maximal tear film concentration is achieved with usage of 20 μl [24]. The remaining amount of the administered eye drop will simply overflow the eye or drain into the nasolacrimal duct. With ageing, the flow of tears will also decrease, which will increase complaints of irritation, especially when applying the topical medication [6]. Due to this, the concentration and absorption into the cornea will decrease through a dilution effect, which will result in a lower response of eye drops in certain subjects, which might lead to an increase in the dose. It is also possible that patients apply their topical medication drop at more than the one drop prescribed in one or both eyes, leading to potential overdose and increased risk of systemic side-effects.
Limitations of the study
One of the limitations of our study is that being a cross-sectional study, the results depend on the recall of falling, which might be sensitive to recall bias. It is reported that 13–32% of interviewed subjects do not remember if they have fallen [35]. This is backed up by the fact that in our study, the number of patients who actually fell in the past 12 months was very low compared to population studies on this topic. Another possible limitation concerns the non-responders, who were older and used slightly more topical beta-blockers, which could lead to selection bias, since the participants may have constituted a healthier group compared to the non-participants.
Side-effects of beta-blockers usually occur shortly after the start of use. Because one of our inclusion criteria was a stable long-term use of IOP-lowering medication over the last year, this may have led to an under-reporting of side-effects. Furthermore, confounding by indication might also play a role: patients with a cardiovascular history are not likely to receive ophthalmic beta-blockers from their ophthalmologist.
All the participants were diagnosed with ocular hypertension or open-angle glaucoma. It is known that one of the complications of glaucoma is visual field loss, which is also one of the many risk factors for falling. However, it is inconclusive whether there is an association between reduced visual fields and increased fall risk [17].
Finally, the total number of subjects was relatively small, and therefore the results may not be significantly associated because of a lack of power (67%). However, the data do not suggest a large difference between the subgroups.
Considering the extensive use of beta-blockers in glaucoma patients worldwide, the number of published case-reports on side-effects is low and mainly focused on cardiovascular adverse events [8, 15]. This might indicate that there is a special subgroup of patients who are at increased risk for these side-effects [e.g., older patients with incident co-morbidity (infection, CVA, weight loss, cardiovascular events, etc.), orthostatic hypotension caused by autonomic dysfunction and/or co-medication]. The underlying mechanism of cardiovascular side-effects is probably cerebral hypoperfusion, especially a transient global cerebral hypoperfusion in syncope [36]. Autonomic failure increases with age, and is probably an important cause of orthostatic hypotension in older patients [37, 38].
Pulmonary side-effects are less frequently reported. Probably patients at risk of these side-effects are more easily identified anamnestically. Lung complaints often can even be observed during the ophthalmic examination (e.g., dyspnoe, wheezing). The cardiovascular risk profile includes heart failure, arrhythmias and changes in serum lipids, which are often not known by the patient himself, and cannot easily be observed during ophthalmic examination. To minimize the risk, a complete pre-treatment cardiovascular examination could be performed; whether this is cost-effective has not yet been investigated.
In summary, we found no increased risk for falls, orthostatic hypotension or dizziness in ophthalmic outpatients on stable long-term use of beta-blocker eye drops. However, we did find a lower baseline pulse rate in rest (supine) and a diminished increase in pulse rate at 1 minute of standing in the subjects on ophthalmic beta-blocker eye-drops, which—in daily life—may contribute to increased fall risk.
Further research in prospective studies with larger numbers of participants is needed to verify our findings, to quantify the incidence of serious adverse events, and to identify the subgroups at risk, especially those at risk of cardiovascular side-effects.
References
Maier PC, Funk J, Schwarzer G, Antes G, Falck-Ytter YT (2005) Treatment of ocular hypertension and open angle glaucoma: meta-analysis of randomised controlled trials. BMJ 331:134
Heijl A, Leske MC, Bengtsson B, Hyman L, Bengtsson B, Hussein M (2002) Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial. Arch Ophthalmol 120:1268–1279
Diggory P, Franks WA (1997) Glaucoma therapy may take your breath away. Age Ageing 26:63–67. doi:10.1093/ageing/26.2.63
Munroe WP, Rindone JP, Kershner RM (1985) Systemic side effects associated with the ophthalmic administration of timolol. Drug Intel Clin Pharm 19:85–89
Novack GD, O'Donnell MJ, Molloy DW (2002) New glaucoma medications in the geriatric population: efficacy and safety. J Am Geriatr Soc 50:956–962. doi:10.1046/j.1532-5415.2002.50226.x
Detry-Morel M (2006) Side effects of glaucoma medications. Bull Soc Belge Ophtalmol 299:27–40
Stewart WC, Garrison PM (1998) Beta-blocker-induced complications and the patient with glaucoma. Newer treatments to help reduce systemic adverse events. Arch Intern Med 158:221–226. doi:10.1001/archinte.158.3.221
Muller ME, van der Velde N, Krulder JW, van der Cammen TJ (2006) Syncope and falls due to timolol eye drops. BMJ 332:960–961
American Geriatrics Society, British Geriatrics Society, and American Academy of Orthopaedic Surgeons Panel on Falls Prevention (2001) Guideline for the prevention of falls in older persons. J Am Geriatr Soc 49:664–672. doi:10.1046/j.1532-5415.2001.49115.x
Leipzig RM, Cumming RG, Tinetti ME (1999) Drugs and falls in older people: a systematic review and meta-analysis: II. Cardiac and analgesic drugs. J Am Geriatr Soc 47:40–50
Leipzig RM, Cumming RG, Tinetti ME (1999) Drugs and falls in older people: a systematic review and meta-analysis: I. Psychotropic drugs. J Am Geriatr Soc 47:30–39
Ziere G, Dieleman JP, Hofman A, Pols HA, van der Cammen TJ, Stricker BH (2006) Polypharmacy and falls in the middle aged and elderly population. Br J Clin Pharmacol 61:218–223. doi:10.1111/j.1365-2125.2005.02543.x
Campbell AJ, Robertson MC, Gardner MM, Norton RN, Buchner DM (1999) Psychotropic medication withdrawal and a home-based exercise program to prevent falls: a randomized, controlled trial. J Am Geriatr Soc 47:850–853
van der Velde N, Stricker BH, Pols HA, van der Cammen TJ (2007) Risk of falls after withdrawal of fall-risk-increasing drugs: a prospective cohort study. Br J Clin Pharmacol 63:232–237. doi:10.1111/j.1365-2125.2006.02736.x
van der Velde N, Ziere G, van der Cammen TJ (2004) Falls in three patients due to timolol eye drops, tolterodine, and flecainide. J Gerontol A Biol Sci Med Sci 59:1343–1344
Everitt DE, Avorn J (1990) Systemic effects of medications used to treat glaucoma. Ann Intern Med 112:120–125
Black A, Wood J (2005) Vision and falls. Clin Exp Optom 88:212–222
van der Valk R, Webers CA, Hendrikse F, de Vogel SC, Prins MH, Schouten JS (2007) Predicting intraocular pressure change before initiating therapy: timolol versus latanoprost. Acta Ophthalmol 86(4):415–418
van der Valk R, Webers CA, Schouten JS, Zeegers MP, Hendrikse F, Prins MH (2005) Intraocular pressure-lowering effects of all commonly used glaucoma drugs: a meta-analysis of randomized clinical trials. Ophthalmology 112:1177–1185. doi:10.1016/j.ophtha.2005.01.042
Campbell AJ, Reinken J, Allan BC, Martinez GS (1981) Falls in old age: a study of frequency and related clinical factors. Age Ageing 10:264–270. doi:10.1093/ageing/10.4.264
The Consensus Committee of the American Autonomic Society and the American Academy of Neurology (1996) Consensus statement on the definition of orthostatic hypotension, pure autonomic failure, and multiple system atrophy. Neurology 46:1470
Wong SN, Tz Sung RY, Leung LC (2006) Validation of three oscillometric blood pressure devices against auscultatory mercury sphygmomanometer in children. Blood Press Monit 11:281–291. doi:10.1097/01.mbp.0000209082.09623.b4
White WB, Herbst T, Thavarajah S, Giacco S (2003) Clinical evaluation of the Trimline blood pressure cuffs with the Accutorr Plus Monitor. Blood Press Monit 8:137–140
Lama PJ (2002) Systemic adverse effects of beta-adrenergic blockers: an evidence-based assessment. Am J Ophthalmol 134:749–760. doi:10.1016/S0002-9394(02)01699-9
Waldock A, Snape J, Graham CM (2000) Effects of glaucoma medications on the cardiorespiratory and intraocular pressure status of newly diagnosed glaucoma patients. Br J Ophthalmol 84:710–713. doi:10.1136/bjo.84.7.710
Kirwan JF, Nightingale JA, Bunce C, Wormald R (2002) Beta blockers for glaucoma and excess risk of airways obstruction: population based cohort study. BMJ 325:1396–1397
Frishman WH, Kowalski M, Nagnur S, Warshafsky S, Sica D (2001) Cardiovascular considerations in using topical, oral, and intravenous drugs for the treatment of glaucoma and ocular hypertension: focus on beta-adrenergic blockade. Heart Dis 3:386–397
Vander Zanden JA, Valuck RJ, Bunch CL, Perlman JI, Anderson C, Wortman GI (2001) Systemic adverse effects of ophthalmic beta-blockers. Ann Pharmacother 35:1633–1637. doi:10.1345/aph.18464
Diggory P, Cassels-Brown A, Fernandez C (1996) Topical beta-blockade with intrinsic sympathomimetic activity offers no advantage for the respiratory and cardiovascular function of elderly people. Age Ageing 25:424–428. doi:10.1093/ageing/25.6.424
Kirwan JF, Nightingale JA, Bunce C, Wormald R (2004) Do selective topical beta antagonists for glaucoma have respiratory side effects? Br J Ophthalmol 88:196–198. doi:10.1136/bjo.2003.017715
Diggory P, Cassels-Brown A, Vail A, Hillman JS (1998) Randomised, controlled trial of spirometric changes in elderly people receiving timolol or betaxolol as initial treatment for glaucoma. Br J Ophthalmol 82:146–149. doi:10.1136/bjo.82.2.146
Leier CV, Baker ND, Weber PA (1986) Cardiovascular effects of ophthalmic timolol. Ann Intern Med 104:197–199
Kaila T, Huupponen R, Karhuvaara S, Havula P, Scheinin M, Iisalo E, Salminen L (1991) Beta-blocking effects of timolol at low plasma concentrations. Clin Pharmacol Ther 49:53–58
Vuori ML, Kaila T (1995) Plasma kinetics and antagonist activity of topical ocular timolol in elderly patients. Graefes Arch Clin Exp Ophthalmol 233:131–134
Cummings SR, Nevitt MC, Kidd S (1988) Forgetting falls. The limited accuracy of recall of falls in the elderly. J Am Geriatr Soc 36:613–616
Brignole M, Alboni P, Benditt D, Bergfeldt L, Blanc JJ, Bloch Thomsen PE, Fitzpatrick A, Hohnloser S, Kapoor W, Kenny RA, Theodorakis G, Kulakowski P, Moya A, Raviele A, Sutton R, Wieling W, Janousek J, van Dijk G (2001) Task force on syncope, European Society of Cardiology. Part 1. The initial evaluation of patients with syncope. Europace 3:253–260. doi:10.1053/eupc.2001.0190
Brignole M, Alboni P, Benditt D, Bergfeldt L, Blanc JJ, Bloch Thomsen PE, Fitzpatrick A, Hohnloser S, Kapoor W, Kenny RA, Theodorakis G, Kulakowski P, Moya A, Raviele A, Sutton R, Wieling W, Janousek J, van Dijk G (2001) Task force on syncope, European Society of Cardiology. Part 2. Diagnostic tests and treatment: summary of recommendations. Europace 3:261–268. doi:10.1053/eupc.2001.0191
Brignole M (2007) Diagnosis and treatment of syncope. Heart 93:130–136. doi:10.1136/hrt.2005.080713
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Additional information
Financial support: None
The authors have full control of all primary data, and agree to allow Graefe's Archive for Clinical and Experimental Ophthalmology to review the data upon request.
No conflicting relationship exists for any author.
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Ramdas, W.D., van der Velde, N., van der Cammen, T.J.M. et al. Evaluation of risk of falls and orthostatic hypotension in older, long-term topical beta-blocker users. Graefes Arch Clin Exp Ophthalmol 247, 1235–1241 (2009). https://doi.org/10.1007/s00417-009-1092-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-009-1092-8