2017-02-01
Contrast-enhanced cardiac magnetic resonance: Distinction between cardiac sarcoidosis and infarction scar
Publication
Publication
Sarcoidosis Vasculitis and Diffuse Lung Diseases , Volume 34 - Issue 4 p. 307- 314
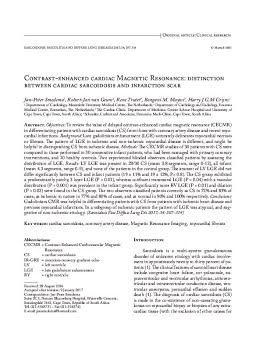
Objectives: To review the value of delayed contrast-enhanced cardiac magnetic resonance (CECMR) in differentiating patients with cardiac sarcoidosis (CS) from those with coronary artery disease and recent myocardial infarctions.
Background: Late gadolinium enhancement (LGE) accurately delineates myocardial necrosis or fibrosis. The pattern of LGE in ischemic and non-ischemic myocardial disease is different, and might be helpful in distinguishing CS from ischemic disease. Methods: The CECMR studies of 30 patients with CS were compared to those performed in 30 consecutive infarct patients, who had been managed with primary coronary interventions, and 10 healthy controls. Two experienced blinded observers classified patients by assessing the distribution of LGE.
Results: LV LGE was present in 29/30 CS (mean 3.8 segments, range 0-12), all infarct (mean 4.3 segments, range 0-9), and none of the patients in the control group. The amount of LV LGE did not differ significantly between CS and infarct patients (19 ± 11% and 19 ± 12%, P= 0.8). The CS group exhibited a predominantly patchy, 3 layer LGE (P = 0.01), whereas confluent transmural LGE (P = 0.04) with a vascular distribution (P < 0.001) was prevalent in the infarct group. Significantly more RV LGE (P = 0.01) and dilation (P = 0.02) were found in the CS group. The two observers classified patients correctly as CS in 72% and 83% of cases, as ischemic in nature in 77% and 80% of cases, and as normal in 90% and 100% respectively.
Conclusions: Gadolinium CMR was helpful in differentiating patients with CS from patients with ischemic heart disease and previous myocardial infarctions. In a subgroup of ischemic patients the pattern of LGE was atypical, and suggestive of non-ischemic etiology.
| Additional Metadata | |
|---|---|
| , , , | |
| hdl.handle.net/1765/105940 | |
| Sarcoidosis Vasculitis and Diffuse Lung Diseases | |
| Organisation | Department of Radiology |
|
Smedema, J.-P., van Geuns, R. J., Truter, R., Mayosi, B., & Crijns, H. (2017). Contrast-enhanced cardiac magnetic resonance: Distinction between cardiac sarcoidosis and infarction scar. Sarcoidosis Vasculitis and Diffuse Lung Diseases (Vol. 34, pp. 307–314). Retrieved from http://hdl.handle.net/1765/105940 |
|