


Abstract
Regular therapy with the radiolabeled somatostatin analog 177Lu-octreotate (22.2–29.6 GBq) in patients with gastroenteropancreatic or bronchial neuroendocrine tumors results in tumor remission in 46% of patients, including minor response. We present the effects of additional therapy with 177Lu-octreotate in patients in whom progressive disease developed after an initial benefit from regular therapy. Methods: Thirty-three patients with progressive disease after an initial radiologic or clinical response were treated with additional cycles of 177Lu-octreotate. The intended cumulative dose of additional therapy was 14.8 GBq in 2 cycles. Responses were evaluated using Southwest Oncology Group criteria, including minor response (tumor size reduction of ≥25% and <50%). Results: Median time to progression (TTP) after regular therapy was 27 mo. In 4 patients, the intended cumulative dose was not achieved (2 had progressive disease, 2 had long-lasting thrombocytopenia). Hematologic toxicity grade 3 was observed in 4 patients, and grade 4, in 1. The median follow-up time was 16 mo (range, 1–40 mo). No kidney failure or myelodysplastic syndrome was observed. Renewed tumor regression was observed in 8 patients (2 partial remission, 6 minor response), and 8 patients had stable disease. Median TTP was 17 mo. Treatment outcome was less favorable in patients with a short TTP after regular cycles. Treatment effects in patients with pancreatic neuroendocrine tumors were similar to those in patients with other gastroenteropancreatic neuroendocrine tumors. Conclusion: Most patients tolerated additional cycles with 177Lu-octreotate well. None developed serious delayed adverse events. Additional cycles with 177Lu-octreotate can have antitumor effects, but effects were less than for the regular cycles. This may be because of a worse clinical condition, more extensive tumor burden, or changed tumor characteristics. We conclude that this salvage therapy can be effective and is safe.
Well-differentiated gastroenteropancreatic neuroendocrine tumors (GEP NETs) usually grow relatively slowly and can produce a variety of bioactive substances such as serotonin, insulin, and so forth, which can lead to hormone-induced symptoms. The incidence is quite low (up to 5/100,000/y for all disease stages), but the prevalence is much higher (35/100,000) (1).
Few effective therapeutic options are available for patients with inoperable or metastasized GEP NETs and bronchial carcinoids. Biotherapy with somatostatin analogs or interferon can result in an improvement of symptoms caused by an excess of bioactive substances, but tumor size reduction rarely occurs (2–4). Chemotherapy with various regimens can result in tumor shrinkage, but the median time to progression (TTP) is usually shorter than 18 mo (5,6). Moreover, such therapies can have significant side effects and an impact on the quality of life.
Peptide receptor radionuclide therapy with the radiolabeled somatostatin analog [177Lu-DOTA0,Tyr3]octreotate (177Lu-octreotate) is a relatively new therapy. It has been used for several years now in our hospital when treating patients with somatostatin receptor–positive tumors that are inoperable or metastasized, of which GEP NETs are the largest group. Treatment with up to 29.6 GBq of 177Lu-octreotate resulted in tumor size reduction of 25% or more in 46% of 310 patients, stable disease was observed in 35%, and progressive disease in 20% (7). Median TTP was 40 mo, and serious side effects such as renal insufficiency or myelodysplastic syndrome occurred in 1% of patients (7). These results compare favorably with those of chemotherapy regimens, although there are no randomized clinical trials at present comparing these modalities.
Several factors are predictive of either tumor regression or tumor progression after therapies with 177Lu-octreotate. The less extensive liver metastases are, and the higher the tumor uptake on pretherapy somatostatin receptor scintigraphy with [111In-DTPA0] octreotide, the better the chances for tumor remission. On the other hand, a poorer clinical condition (i.e., Karnofsky Performance Status [KPS] ≤ 70) and a more extensive tumor load on pretherapy somatostatin receptor scintigraphy are associated with a higher chance that the therapy outcome will be progressive disease (8).
At the moment, it is uncertain which further therapeutic steps are preferable if disease becomes progressive again after an initial response on 177Lu-octreotate. Given the limited options for effective treatments in patients with progressive, well-differentiated GEP NETs, it was a logical step to study the effects of additional treatment cycles of 177Lu-octreotate. Patients with an earlier benefit (i.e., radiologic response or clinical response) from regular treatment with 177Lu-octreotate who later experienced progressive disease received an additional intended cumulative dose of 14.8 GBq. We present the effects of this salvage therapy and discuss both antitumor effects and side effects.
MATERIALS AND METHODS
Patients
Between October 2003 and July 2007, 42 Dutch patients were evaluated for additional therapy with 177Lu-octreotate, of whom 33 patients were treated subsequently and underwent follow-up in our hospital. Before October 2003, the option for additional therapy with 177Lu-ocreotate did not exist. July 2007 was chosen as the final inclusion date for this analysis to allow time for follow-up after finishing additional therapy. All patients had had benefit from prior therapy with 18.5–29.6 GBq of 177Lu-octreotate and later again experienced progressive disease, documented by CT or [111In-DTPA0]octreotide scintigraphy. Benefit was defined as a radiologic tumor response (decrease in tumor size of ≥25%), or, in the absence of a radiologic response, as symptomatic improvement or a decrease of at least 50% in serum chromogranin A (CgA) levels or conversion of proven progressive disease in the 12 mo before the start of regular therapy into stable disease. All patients had measurable disease. All patients had tumor tissue uptake with pretherapy [111In-DTPA0]octreotide scintigraphy that was, on average, equal to or higher than the uptake in normal hepatic tissue on planar images. Patients with known somatostatin receptor–negative lesions were excluded. Prerequisites for treatment were hemoglobin ≥ 5.5 mmol/L, white blood count ≥ 2 × 109/L, platelets ≥ 80 × 109/L, creatinine ≤ 150 μmol/L, creatinine clearance ≥ 40 mL/min, and KPS ≥ 50.
Methods
[DOTA0,Tyr3]octreotate was obtained from Mallinckrodt. 177LuCl3 was obtained from NRG and Missouri University Research Reactor and was distributed by IDB-Holland. 177Lu-octreotate was locally prepared as described previously (9).
Three milligrams of granisetron were injected intravenously as a precaution against nausea. To reduce the radiation dose to the kidneys, an infusion of amino acids (1 L of arginine 2.5% and lysine 2.5%) was started 30 min before the administration of the radiopharmaceutical and lasted for 4 h. Via a second pump system, the radiopharmaceutical was coadministered. Cycle doses of additional therapy were 7.4 GBq (or 3.7 GBq occasionally) injected in 30 min. The interval between treatments was 6–10 wk. Patients were treated up to an intended additional cumulative dose of 14.8 GBq.
Routine hematology, liver and kidney function tests, serum CgA levels, and hormone measurements were performed before each therapy, as well as at follow-up visits. CT or MRI was performed within 3 mo before the first therapy, at 6–8 wk or 3 mo, at 6 mo after the last treatment, and every 6 mo thereafter.
Imaging
After therapy, planar spot images of regions with somatostatin receptor–positive pathology were obtained 24 h after the injection of the therapeutic dose of 177Lu-octreotate. The acquisition time was 7.5 min.
In Vivo Measurements and Response Evaluation
The tumors on CT or MRI were measured and scored according to modified Southwest Oncology Group solid tumor response criteria (10): complete response, complete disappearance of disease; partial remission, ≥50% decrease; minor response, tumor size reduction of ≥25% and <50%; progressive disease, ≥50% increase or new lesion; stable disease, neither complete remission, partial remission, minor response, nor progressive disease. Minor response was added because GEP NETs in general are slow-growing tumors and can be cystic, which makes it unlikely that they respond to treatment similarly to fast-growing solid tumors.
If patients had radiologically stable disease but were in poor clinical condition, this was regarded as treatment failure and scored as progressive disease. Biochemical markers, such as serum CgA levels, were not considered in determining treatment outcome.
The uptake during pretreatment [111In-DTPA0]octreotide scintigraphy was scored visually on planar images using the following 4-point scale: lower than (grade 1), equal to (grade 2), or higher than (grade 3) normal liver tissue; or higher than normal spleen or kidney uptake (grade 4).
Statistics
The Fisher exact test was used to evaluate differences in categoric characteristics and in responses between subgroups of patients. The sign test was used to compare paired (intrapatient) characteristics of patients before starting regular therapy and before starting additional cycles. The Mann–Whitney test for nonnormally distributed variables and a t test were used to compare medians and means. Kaplan–Meier analysis was used to estimate median TTP and median survival. The log-rank test was used to compare these medians in subgroups of patients. For all tests, a P value of less than 0.05 (2-sided) was considered statistically significant.
RESULTS
Forty-two patients were evaluated for the option to receive 2 additional cycles of 177Lu-octreotate at the time of progression after an initial radiologic or clinical response. Nine patients were not eligible: 2 had absent or low tumor uptake on [111In-DTPA0]octreotide scintigraphy. A lung carcinoma had developed in 1 patient as a secondary primary tumor, which probably determined the patient's prognosis. In 4 patients, the clinical condition was so rapidly decreasing and the estimated life expectancy so shortened that further therapy was considered not to be an option. In 1 patient, progressive disease presented as hydronephrosis due to pelvic lymphadenopathy. When the obstruction had been resolved, the clinical condition was no longer sufficient to start therapy with 177Lu-octreotate. To conclude, 1 patient at first was eligible but declined further therapy until the disease progressed further. However, by that time, at the age of 87 y, the patient was no longer eligible because of a decreased clinical condition and insufficient renal function (2 × 24-h urine creatinine clearance at approximately 30 mL/min, serum creatinine of 95 μmol/L).
Thirty-three patients were eligible and received additional therapy with 177Lu-octreotate. The median age at the start of additional therapy was 57 y (range, 35–75 y). Tables 1 and 2 describe baseline characteristics.
Patient Characteristics at Start of Additional Therapy
Additional Patient Characteristics and Comparisons
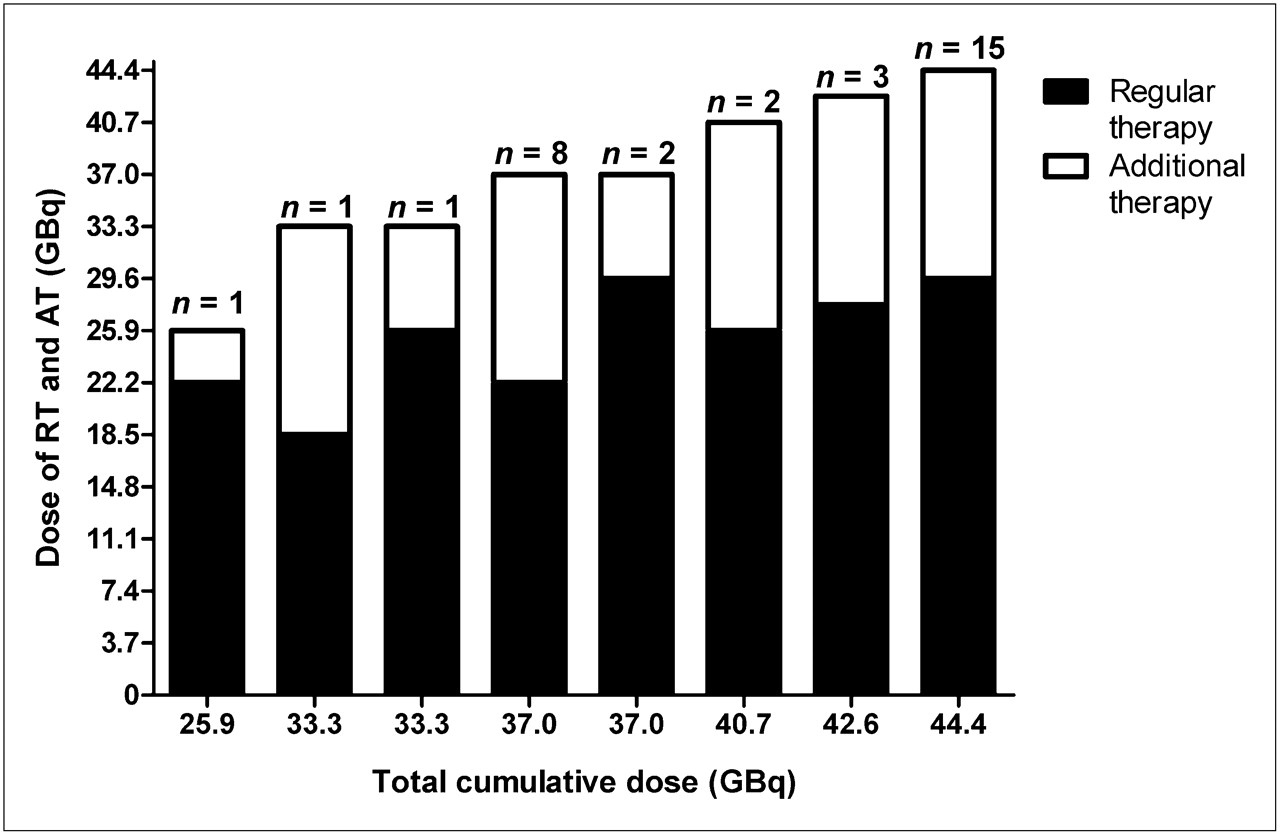
Cumulative doses of 177Lu-octreotate therapies are presented in Figure 1. Thirty patients received 37 GBq or more. The intended dose of 14.8 GBq of 177Lu-octreotate for additional therapy was not reached in 4 of the 33 patients. In 2 patients, disease progressed further after the first cycle: 1 patient started with chemotherapy because of clinical and radiologic progression, and the other patient, after an initial clinical improvement, died 6 wk after the additional treatment was started, presumably because of progressive disease. In 2 other patients, persistent myelotoxicity after 3.7 and 7.4 GBq of 177Lu-octreotate made further additional therapy impossible.
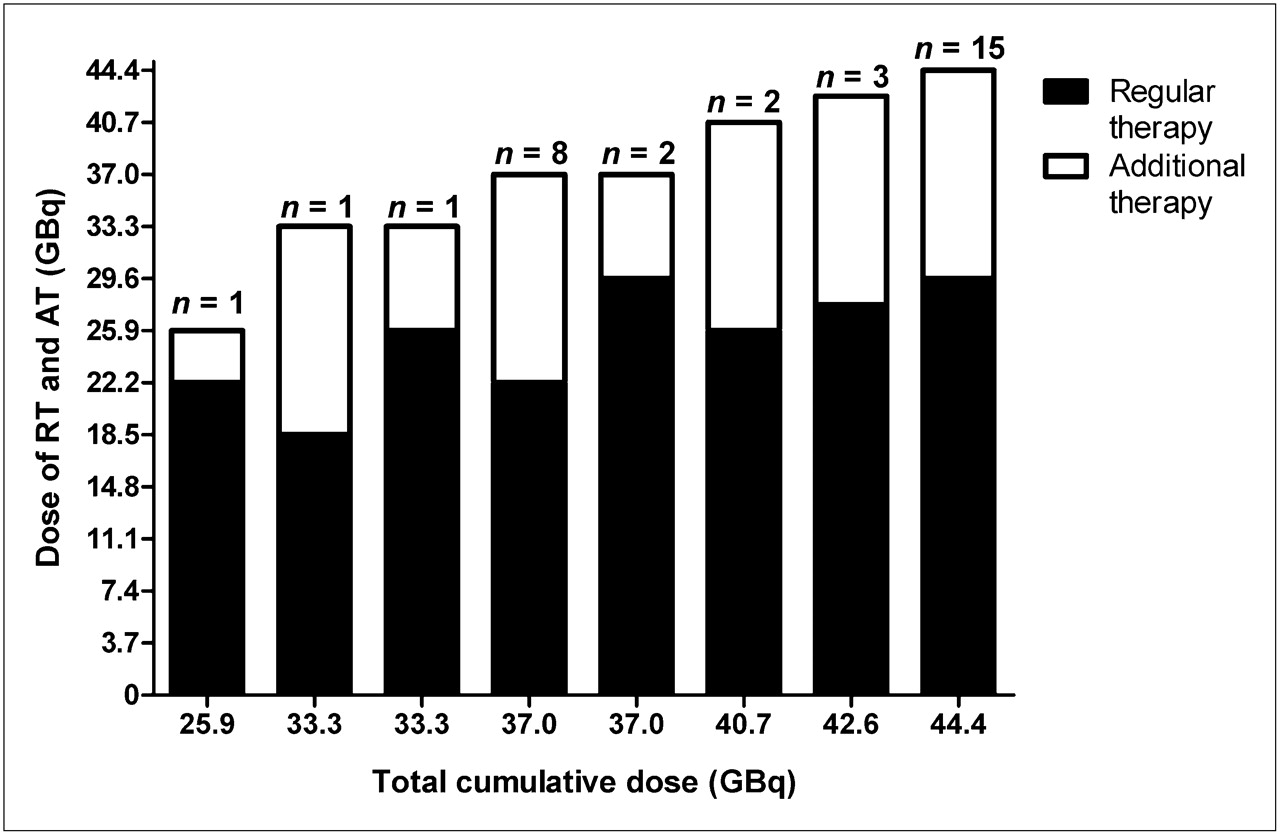
Dose of cumulative administered activity of 177Lu-octreotate. AT = additional therapy; RT = regular therapy.
Table 2 describes baseline patient characteristics for the entire group of 310 patients who received regular therapy with 177Lu-octreotate and for the 33 patients who received additional therapy later. In the latter group, baseline characteristics are presented both from the start of regular therapy and from the start of additional therapy. The patients who later received additional cycles had a different distribution of the amount of tumor uptake on pretherapy somatostatin receptor scintigraphy at the start of regular therapy compared with all 310 treated patients (Fisher exact test: P < 0.05). Grade 4 tumor uptake was present more often. More patients who later received additional cycles had an elevated baseline value of alkaline phosphatase of more than 120 U/L (74% vs. 55%); this difference was close to being statistically significant (Fisher exact test: P = 0.06).
In patients who received additional cycles, more patients had weight loss at the start of additional therapy (Fisher exact test: P < 0.05). More patients had bone metastases, and median CgA and median alkaline phosphatase were more elevated at the start of additional therapy, but these differences were not statistically significant. The median KPS at the start of regular therapy was 100 and at start of additional therapy was 80. This was statistically significant (sign test: P < 0.01).
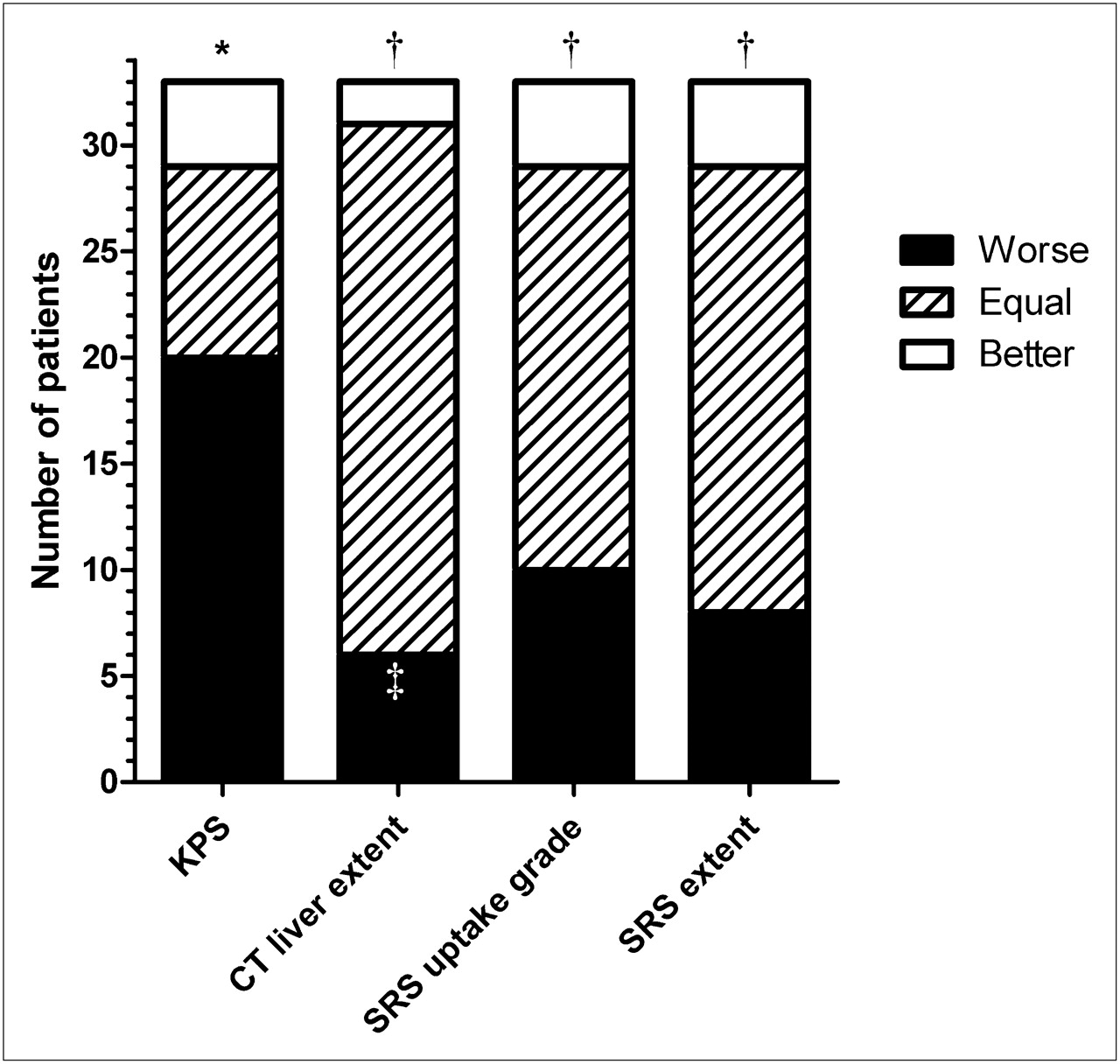
Figure 2 demonstrates, on an intrapatient base, differences in KPS, liver involvement on CT, and extent of disease and tumor uptake on [111In-DTPA0]octreotide scintigraphy from the start of regular treatments to the start of additional treatments.
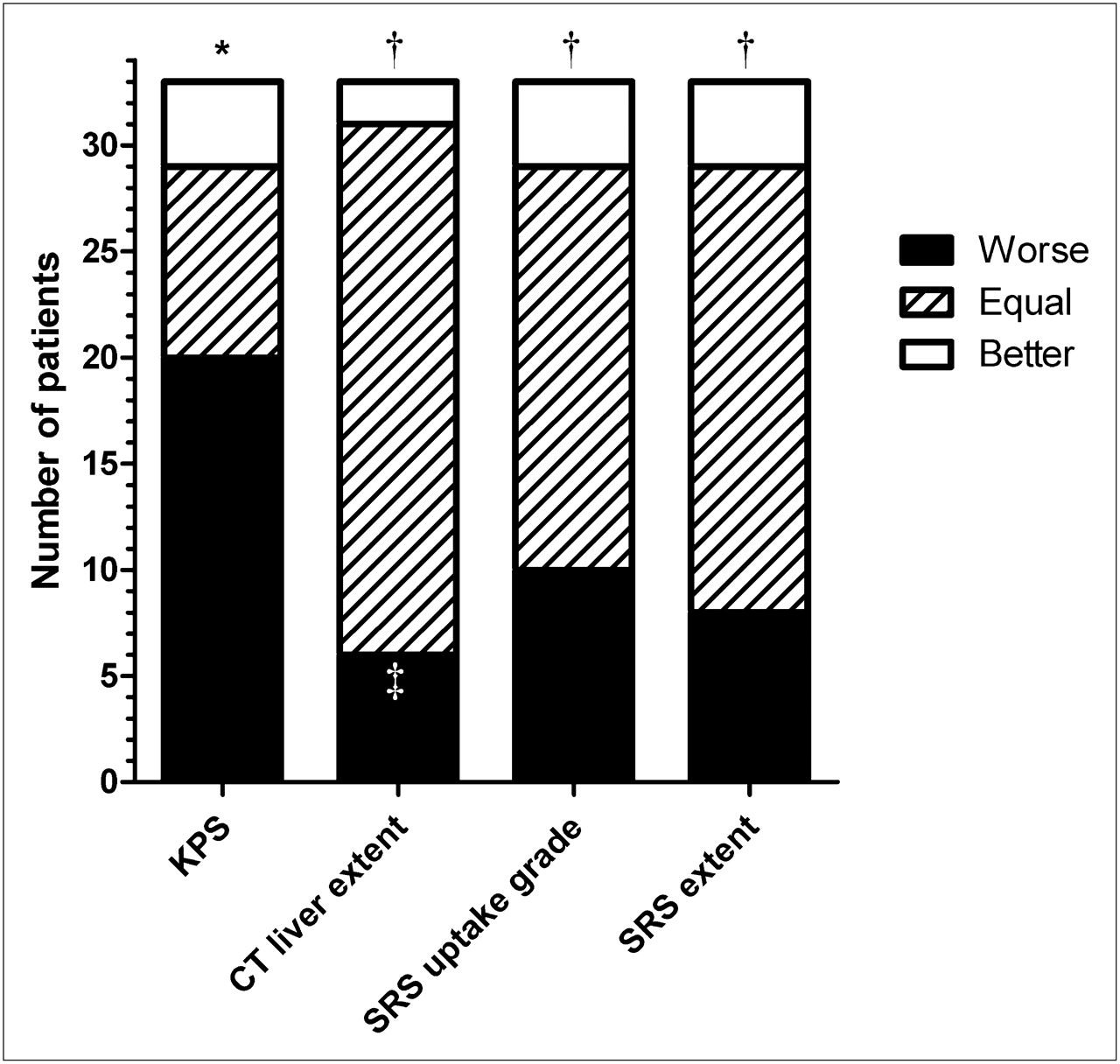
Intrapatient comparison of changes in baseline characteristics from start of regular therapy to start of additional therapy with 177Lu-octreotate. *P < 0.01 (sign test). †Not significant (sign test). ‡Liver metastases not present with regular therapies developed in 4 patients (1 already very diffuse); extensive liver disease developed in 2 with limited lesions. SRS = somatostatin receptor scintigraphy.
Subacute hematologic side effects of the additional cycles with 177Lu-octreotate are presented in Table 3. In one patient with grade 3 thrombocytopenia after regular therapy, the platelet count decreased from 189 to 100 × 109/L after the first additional cycle of 7.4 GBq. Therefore, the dose of the second cycle was reduced to 3.7 GBq. No further significant decrease occurred in platelet count, and finally 3.7 GBq were given again without further toxicity.
Hematologic Toxicity
Of the 4 patients with thrombocytopenia of ≤75 × 109/L, grade 3 or more anemia, or leukocytopenia after regular therapy, 2 patients (50%) experienced grade 3 or more hematologic toxicity after additional therapy, and in 1 patient no follow-up was available because the patient died as a result of progressive disease after the first additional cycle. Of the 29 patients without hematologic toxicity after regular therapy as defined previously, 3 patients (10%) experienced grade 3 or more hematologic toxicity after additional therapy, and in 1 no follow-up was available because of progressive disease after the second cycle.
In no patients did myelodysplastic syndrome or kidney failure develop during the time of follow-up. One patient underwent a nephrectomy after the regular therapy because of renal cell carcinoma. He subsequently was treated with 2 additional cycles of 177Lu-octreotate, with no renal failure noted after more than 2 y of follow-up. The median time of follow-up in the entire group of patients was 15.5 mo after the first additional cycles (range, 1–40 mo). This was 21 mo in the patients with at least stable disease after additional therapy. Since the start of regular therapy, the median time of follow-up for all patients was 44 mo.
Table 4 summarizes the therapy outcome in the 33 studied patients. In 2 patients (6%) the additional cycles of 177Lu-octreotate resulted in a partial remission, and in 6 (18%), in a minor response. Ten additional patients (30%) had radiologically stable disease after additional therapy, but 2 of those had clear clinical signs of progression (development of ascites, decrease in general condition). This was hence considered to be progressive disease as well. Therefore, 8 patients (24%) had stable disease after additional therapy, and in 17 patients (52%) disease remained progressive despite additional therapy. The median TTP after the start of additional therapy in the 16 patients with stable disease, minor response, or partial remission was 17 mo (Kaplan–Meier method, 2 patients censored at 21 mo). Figure 3 shows the disease course in 1 of the patients who responded favorably to both the regular and the additional therapy cycles.

Disease course in patient having carcinoid with liver metastases, presenting imaging studies, serum CgA levels, and body weight over time. Patient had severe diarrhea in 2001 with good clinical, scintigraphic, and radiologic responses after regular therapy with 177Lu-octreotate in 2001. In March 2005, disease became progressive, but patient declined therapy. In December 2006, disease clearly progressed, and additional therapy with 177Lu-octreotate was started. Patient again had partial remission and was still in remission 21 mo after additional therapy.
Therapy Outcome
CgA levels were measured at various moments during the disease course. Only patients with elevated CgA levels at the start of regular therapy and at the start of additional therapy who had follow-up levels after additional therapy are included in the data shown in Figure 4. These included 23 patients, of whom 11 had progressive disease, 6 had stable disease, and 6 had minor response or partial remission after additional therapy. The figure shows that almost all patients had a clear decrease in CgA levels after regular therapy and a clear increase at the time of renewed disease progression before additional therapy. After additional therapy, CgA levels decreased mainly in the patients with a minor response or partial remission.
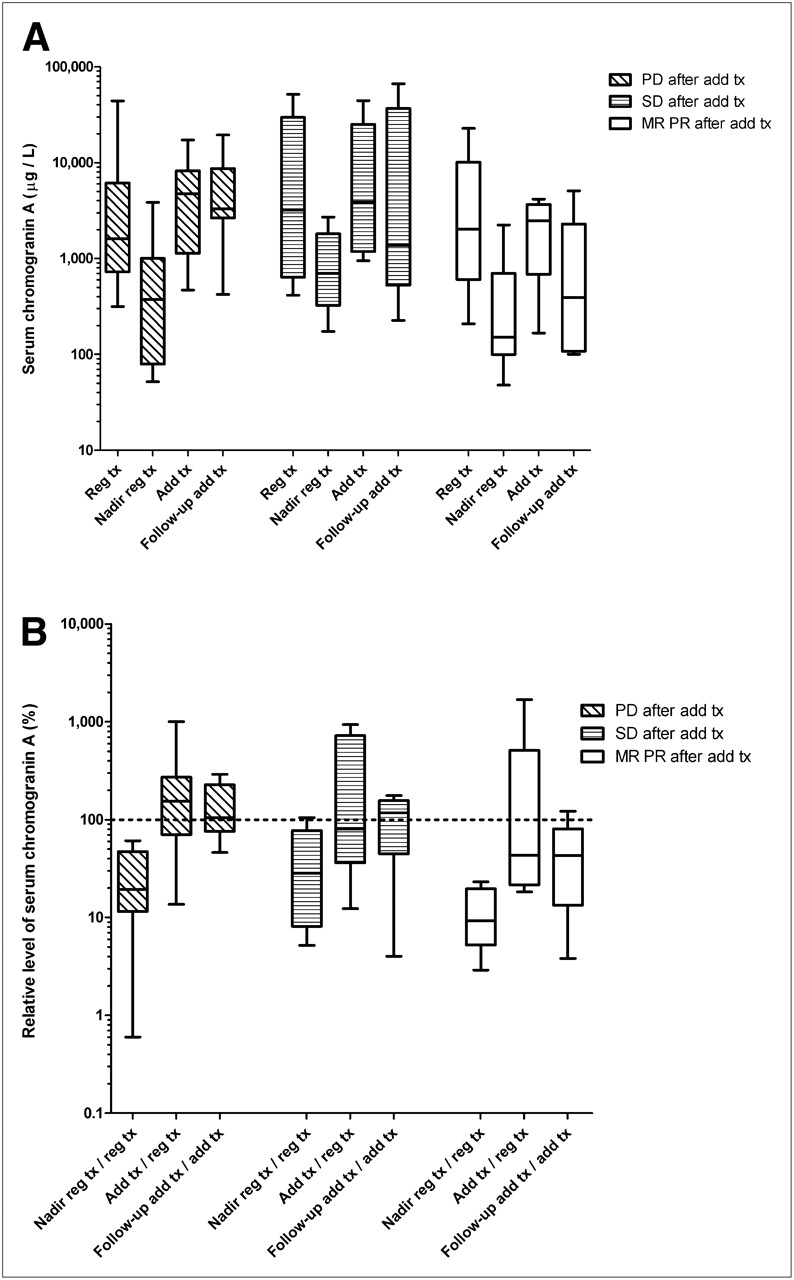
CgA levels in serum during course of disease. (A) Absolute CgA levels at various moments according to treatment outcome of additional therapy. (B) Relative levels of CgA, displaying change after regular therapy (ratio of nadir of CgA after regular therapy over CgA at start of regular therapy), before start of additional therapy (ratio of CgA at start of additional therapy over CgA at start of regular therapy), and after additional therapy (CgA level at follow-up after additional therapy over CgA at start of additional therapy). No change is indicated by 100%. Boxes show medians and 25th−75th percentiles; whiskers indicate ranges. Middle lines in boxes indicate medians. Add tx = additional therapy; MR = minor response; PD = progressive disease; PR = partial remission; Reg tx = regular therapy; SD = stable disease.
The median overall survival since the start of additional cycles was 15 mo. In patients with progressive disease after additional therapy, the median overall survival was 9 mo, and in the patients with stable disease or regression it was 26 mo (log-rank test: P < 0.0001).
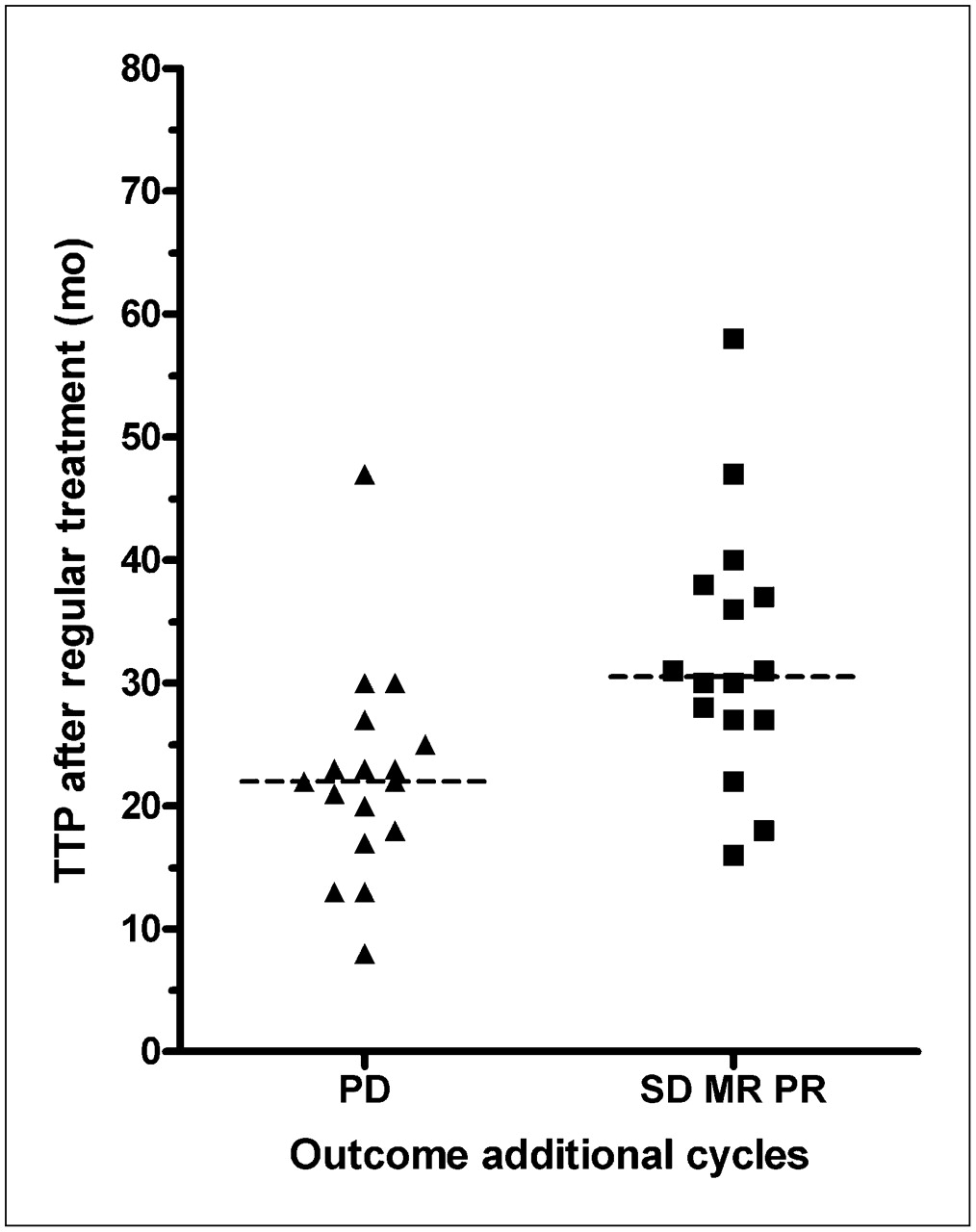
The median TTP after regular therapy was 27 mo in the 33 patients who received additional cycles. In the 16 patients with a TTP of less than 27 mo, 13 (81%) still had progressive disease, 1 (6%) had stable disease, and 2 (13%) had a minor response. In the 17 patients with a TTP of 27 mo or more, 4 patients (24%) still had progressive disease, 7 (41%) had stable disease, 4 (24%) had a minor response, and 2 (12%) had a partial remission. Treatment outcome defined as progressive disease or nonprogressive disease was significantly different between the patients with a TTP of less than 27 mo after regular therapy and those having a TTP of 27 mo or more (Fisher exact test: P < 0.01). The median TTP after regular therapy in patients who continued to have progressive disease was 22.0 mo (mean, 22.47 mo), whereas it was 30.5 mo (mean, 32.25) in patients with stable disease or tumor shrinkage (t test: P < 0.01) (Fig. 5). Of note, 15 of 16 patients (94%) with a TTP of less than 27 mo had an elevated level of alkaline phosphatase at the start of additional therapy, as opposed to 10 of 17 patients (59%) with a TTP of 27 mo or more (Fisher exact test: P < 0.05).
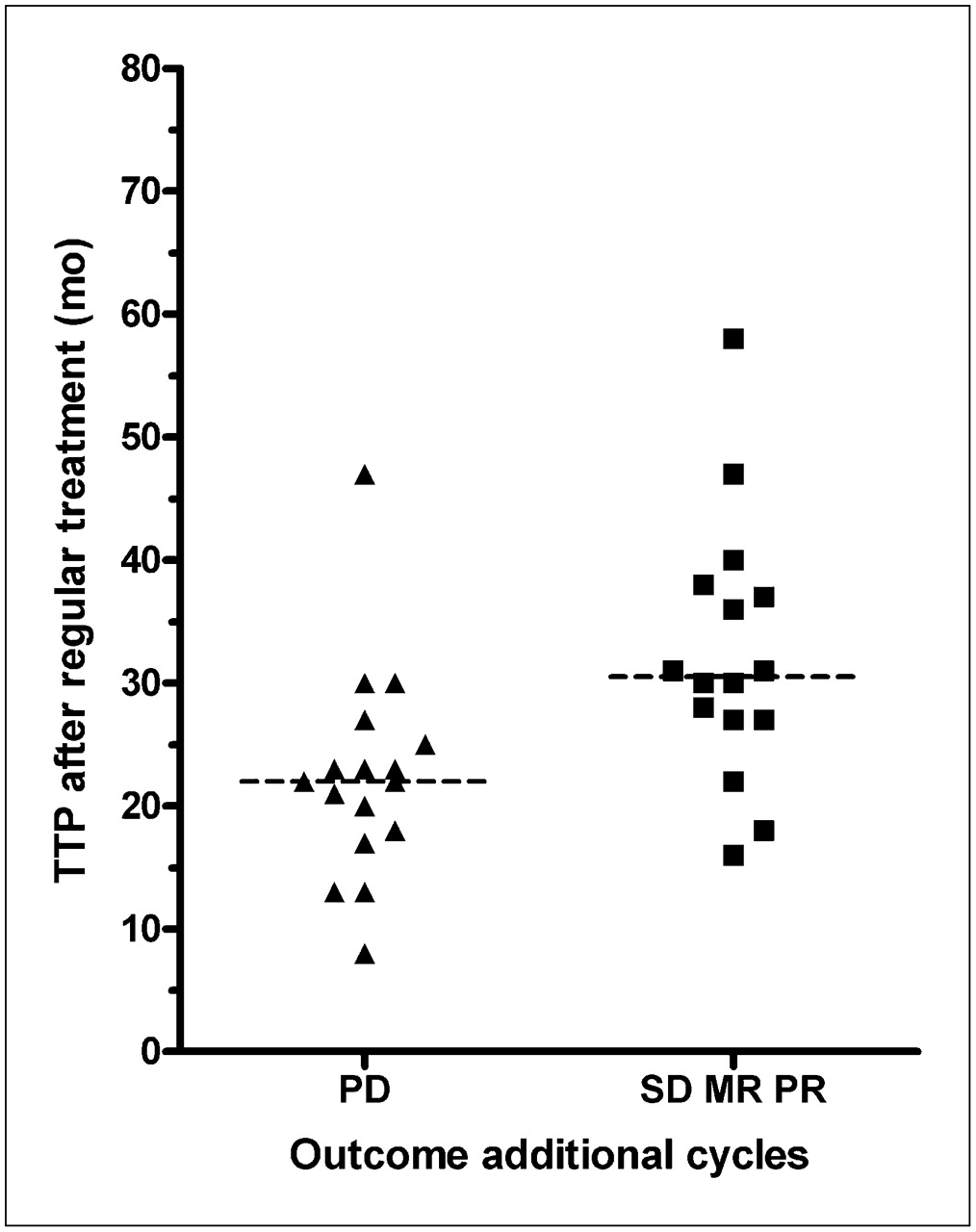
Outcome after additional therapy with 177Lu-octreotate in relation to duration of response after regular therapy. Median TTP (indicated by line) after regular therapy in patients with progressive disease (PD) was 22 mo. This was 30 mo in patients with stable disease (SD) or remission (t test: P < 0.01). MR = minor response; PD = progressive disease; PR = partial remission.
Sixteen of the 23 patients (70%) with elevated levels of alkaline phosphatase at the start of additional cycles still had progressive disease, whereas 1 of the 10 patients (10%) with a normal alkaline phosphatase level still had progressive disease (Fisher exact test: P < 0.01).
The median TTP after regular therapy was 26 mo in pancreatic NET patients (n = 8) and 27 mo in carcinoid patients, including those having NET of an unknown primary source (n = 25). After additional therapy, 5 patients (63%) with pancreatic NET still had progressive disease; and in carcinoid patients, 12 (48%) had progressive disease. The proportion of progressive disease and nonprogressive disease in carcinoid patients and pancreatic NET patients was not significantly statistically different (Fisher exact test: P = 0.69). The median TTP in patients with pancreatic NET was 17 mo and in patients with carcinoid tumors was 20 mo (log-rank test: P = 0.26).
DISCUSSION
Peptide receptor radionuclide therapy with radiolabeled somatostatin analogs such as 177Lu-octreotate is a promising treatment in patients with somatostatin receptor–positive NETs. Initial treatment with 177Lu-octreotate can result in prolonged antitumor effects; however, disease will eventually become progressive again in most patients. We analyzed the effects of additional treatment cycles with 177Lu-octreotate (intended dose of 14.8 GBq) in patients with progressive disease after an initial radiologic or clinical response with 18.5–29.6 GBq of 177Lu-octreotate.
The decision to administer an intended dose of 2 cycles of 7.4 GBq was made to try to avoid long-term side effects. The intended cumulative dose of the regular treatment was based on the estimation that 29.6 GBq of 177Lu-octreotate would result in a bone marrow dose of 2 Gy (9). If individual dosimetry had indicated that the kidney dose then would be more than 23 Gy, the intended dose was reduced. Probably these assumptions for bone marrow and kidney doses were safe because serious side effects were infrequent (7). When deciding to start the additional therapies, we did not want to exceed these maximum doses for external beam radiotherapy by very much at one time.
In the 33 patients treated with additional cycles of 177Lu-octreotate, renewed tumor remission was observed in 8 and disease stabilization in 8, with a median TTP of 17 mo. In 17 patients, disease remained progressive. The treatment outcome was more favorable in patients who had a long-lasting benefit from regular therapy. Grade 3 or 4 acute hematologic toxicity occurred in 5 patients (15%), somewhat more than the 9.5% of patients in which it occurred after the regular therapy. Apparently patients with myelotoxicity after regular cycles were more susceptible to hematologic toxicity after additional therapy. In these patients, it may be advisable to start additional therapy with 3.7 GBq.
None of the patients experienced serious long-term side effects during follow-up: kidneys and bone marrow are the organs at risk, but kidney failure or myelodysplastic syndrome did not occur after additional therapy with 177Lu-octreotate. However, the overall time of follow-up was relatively short, partly because some patients who had continued progressive disease were lost to follow-up or died shortly after therapy.
Although the additional therapy is safe and can result in tumor stabilization and tumor remission, the antitumor effects are less favorable than with the initial treatments. Several factors may play a role. First, the administered activity for the additional therapy is only half that used in regular treatment, which will result in a lower radiation dose to the tumors.
Another important factor may be that most patients had a worse clinical condition (e.g., lower KPS, weight loss) at the start of additional treatment than at the start of regular treatments. Moreover, some patients had more extensive tumors when starting additional treatment cycles: 4 of 5 patients without hepatic metastases at the start of regular treatments had liver lesions when starting additional cycles. This is important because the extent of tumor spread was a predictive factor for disease progression after therapy (8). Although not statistically significant, several other factors were also higher at the start of additional therapy: the percentage of patients with bone metastases, the median serum CgA, and the median alkaline phosphatase. Elevated alkaline phosphatase levels were an important adverse prognostic factor for survival in patients with metastasized NETs (11).
High tumor uptake on [111In-DTPA0]octreotide scintigraphy was a predictive factor for tumor remission after regular therapy (8). An explanation for the less favorable results could be a decrease in the amount of tumor uptake of the radiolabeled somatostatin analog, either by a decrease in somatostatin receptor expression or by a change in the profile of receptor subtypes. Although we could not demonstrate a statistically significantly lower tumor uptake on 111In-octreotide scintigraphy at the start of additional cycles using a visual score (grades 2–4), a few patients had grade 4 uptake when starting regular treatments and only grade 3 when starting additional cycles. It would be interesting to perform a separate study of tumor dosimetry based on posttherapy scintigraphy results to more precisely determine possible differences in uptake.
Tumor dedifferentiation may also play a role. As tumors become more poorly differentiated over time, somatostatin receptor expression can become less (12), and tumors can start to proliferate more rapidly. One patient had somatostatin receptor–negative vertebral lesions that became apparent shortly after finishing the additional treatment. In another patient who had a pancreatic NET, rapidly progressive liver metastases developed, and additional therapy with 177Lu-octreotate was ineffective. Retrospectively, performing a biopsy to determine the proliferation index (or Ki-67 index) and considering chemotherapy in case of a high index may have been better.
Another factor can be that the patients who so far received additional treatment with 177Lu-octreotate may have had more aggressive tumors at baseline than the average patient treated. In the group of patients who received additional treatments, the median TTP after regular therapy was 27 mo, whereas in the whole group it was 40 mo.
Another group also investigated additional therapy with radiolabeled somatostatin analogs in patients in whom progressive disease again developed after successful regular therapy. Forrer et al. (13) described the effects of 1 cycle of 7.4 GBq [177Lu-DOTA0-Tyr3]octreotide after regular therapy with [90Y-DOTA0-Tyr3]octreotide in 27 patients. They found no serious acute or subacute side effects. At 8–12 wk after therapy, 8 patients (30%) still had progressive disease, 12 (44%) had stable disease, 5 (19%) had a minor response, and 2 (7%) had a partial remission. There were no exact data on the duration of response: 13 patients progressed after a mean of 8.3 mo, and 8 patients still were without progressive disease at the time of analysis. In our view, it is difficult to state exactly what these data mean given the low administered activity and relatively short time of follow-up.
The main limitations of our study are the limited time of follow-up and the small number of treated patients. However, on the basis of our study results, we are convinced the additional cycles can be worthwhile and are safe in most patients. However, it is important to consider other therapeutic options, especially if disease became progressive soon after the regular therapy cycles. Therapy with RAD001 (everolimus) and octreotide could become an alternative: the tumor-stabilizing effects of this combination were promising, although tumor remissions were rare (14). In patients with rapidly progressive disease, etoposide and cisplatin could be an option.
CONCLUSION
Additional treatments with 177Lu-octreotate were well tolerated in most patients who responded favorably to regular treatment and eventually had renewed progressive disease. Hematologic toxicity was rare, and no serious delayed adverse events were observed, although the duration of follow-up was still limited. This salvage therapy can result in tumor stabilization and regression, but results were less favorable than those for the initial treatments. This fact might be a result of the lower amount of administered activity, the decreased clinical condition of patients, changed tumor characteristics, and higher tumor burden.
Acknowledgments
We thank all personnel from the departments of Nuclear Medicine and Internal Medicine, especially research nurses Agnes Keursten, Daniëlle Verwaal, Els Montijn, and Carla van der Pluijm, for their expert help and cooperation.
Footnotes
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication July 31, 2009.
- Accepted for publication December 10, 2009.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}